Re-thinking What Happens When We Touch.

Touch isn’t just physical, it’s perceptual, emotional, and deeply communicative. For manual therapists, this should change everything.
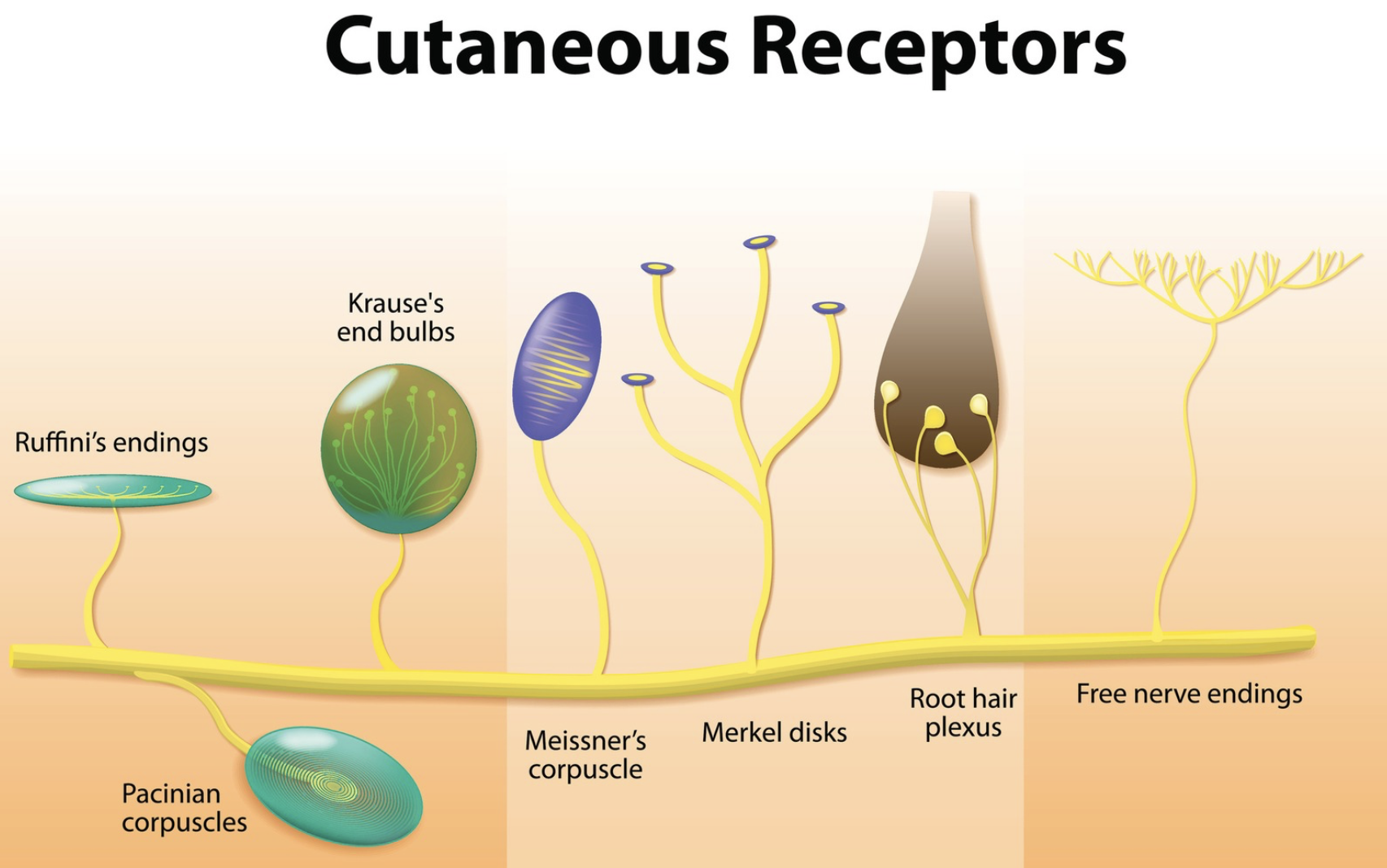
Every time we place a hand on a client, we activate a complex interaction between skin and underlying tissues, sensory nerves, and brain. Mechanoreceptors in the skin and below respond to different types of touch: stretch, vibration, pressure, and temperature. These are involved in tactile discrimination, touch that helps us identify texture, shape, and movement location. It’s the type of touch used when you reach into your pocket to find a coin. It answers the questions: where, what, and how?
But there's another system we often overlook, the C tactile (CT) afferents. These slow conducting sensory fibres are tuned specifically to gentle, affective touch. They don’t help locate or map physical features. Instead, they deliver a different message entirely: this touch feels safe. CT afferents are linked with interoception, the brain's way of sensing what’s happening inside the body, and influence emotional processing, co-regulation, and social bonding. Where tactile discrimination gives the body data, CT input gives the brain meaning.
So what does this mean in practice? When we apply touch that’s slow, intentional, and grounded in presence, we’re speaking directly to the client’s brain in a language of safety and connection. That’s why, even without firm pressure or structural change, a client can feel more at ease. Sometimes, simply placing a hand on a painful area introduces a new, non-threatening input that invites the brain to reassess the perceived danger. The result? Reduced muscle guarding, emotional regulation, and a more coherent body sense.
This isn't to say that pressure based or force based manipulation (FBM) has no role. These techniques can produce temporary local changes, such as changes to circulation or reduced muscle tone, and for some clients, they’re helpful. But responses vary widely depending on age, health status, neurophysiological sensitivity, and previous experiences. This is why pressure alone can’t be the foundation of therapeutic touch. It’s not about what we do to the tissue, but how the client interprets what we do.
And that’s where contextual variables come in, those subtle, often invisible influences that shape outcomes. These include everything from the therapist’s tone of voice, confidence, body language, and facial expression, to the clinical environment, client expectations, beliefs, and the quality of therapeutic rapport. All of these variables contribute to whether the client’s brain perceives the interaction as safe or threatening.

When we frame touch as a mechanical fix, we risk reinforcing outdated, patho-anatomical narratives, stories about fascia being ‘stuck’, joints being ‘out’, or pain being caused by a structural fault. But neuroscience offers a different story. Most persistent pain is not caused by tissue damage. It’s shaped by meaning, memory, and protective prediction, brain driven processes that help the body manage perceived threat. This is particularly true in nociplastic pain, a pain category recognised by the IASP, where pain persists without clear evidence of tissue damage.
Nociplastic pain is real, distressing, and deeply misunderstood. It is not imagined or psychological, it is a reflection of a sensitised nervous system operating in protective overdrive. Telling clients they are broken or that their fascia is dysfunctional or restricted only worsens this. Instead, therapeutic touch offers an opportunity to introduce new, safe experiences that may help recalibrate threat perception.
We see this frequently in clinic where clients are told 'everything looks normal' on scans, yet their pain remains. Rather than invalidating their experience or searching for unseen restrictions, we need to honour their story, understand their system, and shift our thinking. It’s not about what’s wrong in the tissues, it’s about what the nervous system is trying to protect against.
From this perspective, hands on therapy becomes a form of communication. It becomes about presence, timing, intention, and co-regulation. It becomes about trust, not technique. And it becomes clear that therapeutic change is more than tissue deep.
 Our hands don’t need to fix. They need to listen. They need to speak safety. And they need to work with, not on, the person in front of us.
Our hands don’t need to fix. They need to listen. They need to speak safety. And they need to work with, not on, the person in front of us.
It’s time to let go of rigid biomechanical models. Let’s embrace a biopsychosocial, interoceptive, and brain informed understanding of touch. Because when we understand what happens when we touch, we don’t just change symptoms, we support recovery, regulation, and resilience.
References
E. Cook et al., “Developing Manual Therapy Frameworks for Dedicated Pain Mechanisms,” JOSPT Open, vol. 1, no. 1, pp. 48–62, Jul. 2023, doi: 10.2519/josptopen.2023.0002.
J. Draper-Rodi, D. Newell, M. F. Barbe, and J. Bialosky, “Integrated manual therapies: IASP taskforce viewpoint,” Pain Rep, vol. 9, no. 6, p. e1192, Oct. 2024, doi: 10.1097/PR9.0000000000001192.
S. Roura, G. Álvarez, I. Solà, and F. Cerritelli, “Do manual therapies have a specific autonomic effect? An overview of systematic reviews,” PLoS One, vol. 16, no. 12, Dec. 2021, doi: 10.1371/JOURNAL.PONE.0260642.
van Griensven H and Strong J, Pain. A Textbook for Health Professionals, 3rd ed. Elsevier, 2023.
Lin et al., “Patient-centred care: The cornerstone for high-value musculoskeletal pain management,” Nov. 01, 2020, BMJ Publishing Group. doi: 10.1136/bjsports-2019-10191
Singh and A. Chanda, “Mechanical properties of whole-body soft human tissues: A review,” Nov. 01, 2021, IOP Publishing Ltd. doi: 10.1088/1748-605X/ac2b7a.
D. Deflorio, M. Di Luca, and A. M. Wing, “Skin and Mechanoreceptor Contribution to Tactile Input for Perception: A Review of Simulation Models,” Front Hum Neurosci, vol. 16, p. 862344, Jun. 2022, doi: 10.3389/FNHUM.2022.862344/BIBTEX
.J. E. Bialosky et al., “Unraveling the mechanisms of manual therapy: Modeling an approach,” Journal of Orthopaedic and Sports Physical Therapy, vol. 48, no. 1, pp. 8–18, 2018, doi: 10.2519/jospt.2018.7476.H.
Olausson, Wessberg J, I. Morrison, and F. McGlone, Affective touch and the neurophysiology of CT afferents. Springer, 2016.
